Transitional Payment Model (TPM) Information
Last updated March 13, 2025
The Transitional Payment Model (TPM) is a new payment model for eligible Saskatchewan family physicians that combines the existing fee-for-service (FFS) structure with a new capitation payment (based on patient contacts and panel size).
TPM recognizes and supports the delivery of longitudinal community-based family medicine by:
- Promoting longitudinal care within family medicine;
- Acknowledging patient complexity and the additional time required to provide care; and
- Increasing patient access to primary care.
The new model is a transitional step between the current fee-for-service model and the future goal of establishing a blended capitation model as recommended by the Primary Care Compensation Working Group (PCCWG), a collaborative working group formed between the Saskatchewan Medical Association (SMA), Saskatchewan Health Authority (SHA) and the Ministry of Health.
TPM is available to physicians as of April 1, 2024.
1. Eligibility
To be eligible for the program, fee-for-service family physicians must:
- Be licensed to practice and currently reside in Saskatchewan.
- Provide longitudinal family medicine as the majority of their practice in a Saskatchewan community.
- Hold SHA appointment/privileges.
- Commit to being the “Most Responsible Provider” (MRP) to a panel of patients and document patient understanding of the relationship.
- Commit to providing chronic disease management including submitting CDM-QIP flow sheets.
- Provide comprehensive care and on-call services.
- Participate as part of a group (a clinic group or multiple clinic groups for solo physicians) to ensure adequate service and call coverage; and
- Assign a family physician as the physician group lead.
2. Registration
Registration is open on April 19, 2024, and there is no deadline to apply. To qualify for payment for any given quarter you must register within 60 days from the start of each quarter (i.e., May 30 for Q1 or July 30 for Q2).
The deadline to qualify for the first quarter payment has been extended to June 21st due to the delay in the launch of the registration site.
3. Payments
Eligible physicians will receive a payment of up to $144,000 based on the following formula:

Patient Contact Ratio
A patient contact represents each time a physician provides primary care (in-person or via virtual care) to a patient. The visit is considered one contact based on date regardless of the number of services provided during the visit (contact count is limited to one contact per patient per day).
Physician billing data is used to determine the number of patient contacts. The contact ratio is calculated using a threshold of 6,500 contacts.
Patient Panel Ratio
A patient panel is a group of patients assigned to one specific physician.
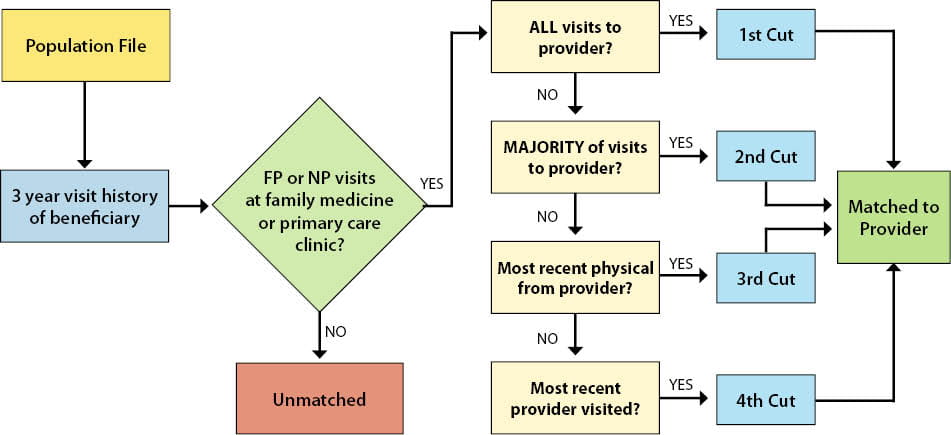
Patient panel size is calculated using a four-cut methodology that matches patients to one physician. The four-cut matching methodology uses a three-year data analysis period to match Saskatchewan patients to a Family Physician or Nurse Practitioner where most of their primary care services were billed to the Medical Services Branch (MSB).
The Patient Panel Ratio is calculated using a threshold panel size of 1,600.
NOTE: An individual physician must have a minimum of 250 patients matched to be eligible for the program.
NOTE: Although the calculations of the ratios use thresholds (6,500 contacts and 1,600 patients), there is no limit on the number of contacts or matched patients a physician may have.
Establishing A Patient Panel
Family physicians are expected to engage in a conversation with their patients about physician-patient empanelment and what a "Most Responsible Physician" (MRP) relationship between physician and patient entails. An empanelment process will be developed by Ministry of Health and the Saskatchewan Medical Association.
- The empanelment process represents a physician’s commitment to delivering patient-centred care by communicating and collaborating with patients regarding the management of their condition(s) and care plan(s) on an on-going basis.
- The empanelment process means the patient commits to seeking all their primary care from that physician, or that physician’s colleague(s) whenever possible.
Physicians will be required to maintain an up-to-date list of empaneled patients as well as to retain copies of all physician-patient documentation. The empaneled patient list will inform the next phases of the Saskatchewan made blended capitation model.
NOTE: For the purposes of calculating TPM payments, the four-cut methodology described in the payment section is used to determine patient panel size, not the number of patients the physician empanels through an established empanelment process.
4. Accountabilities and Deliverables
Physicians participating in TPM are expected to provide the following four deliverables:
1. Establish a longitudinal relationship with patients, by providing ongoing community-based family medicine services to a dedicated patient panel, which includes screening, prevention activities, chronic disease management and comprehensive care.
- When the empanelment process is developed, physicians will be expected to document patient understanding and consent to the Most Responsible Physician (MRP) relationship with each empaneled patient.
- Physicians are expected to provide Chronic Disease Management (CDM) and adhere to best practices in chronic disease managment including the completion and submission of CDM-QIP flowsheets.
- Physicians are expected to provide comprehensive care to their empaneled patients shared by a TPM clinic/group, including hospital and supportive care, nursing home care, pre- and post-natal and infant care, complete physicals including PAP smears, and phone calls from Allied Health Care Providers (AHCP), where applicable.
- Physicians are expected to adhere to a set of Primary Care Quality Indicators once jointly developed by the SMA and Ministry.
- Physicians are expected to adhere to common work standards for EMR/eHR patient-centred information exchange.
2. Commitment to transition towards the Patient’s Medical Home (PMH) framework:
- Physicians are expected to be part of a group with more than one Most Responsible Physician (MRP) participating in TPM.
- For solo clinics, joining a group of physicians (minimum of two family physicians) in the same community or catchment area is encouraged, with all physicians willing to share patient information for coverage and comprehensive care.
- Appointment of at least one family physician lead from the clinic or group to be a point of contact, attend learning events, and liaison with SHA. This role is paid.
- Providing on-call coverage for the group’s patients.
3. Commitment to address multiple relevant patient issues/concerns during one visit.
4. Commitment to any necessary data tracking, sharing, and reporting that demonstrates improvements to primary care delivery and patient outcomes as jointly developed by the SMA and Ministry.
Further details on each deliverable are available.
5. Frequently Asked Questions
Enrolment and Changes to Enrolment
Who can enrol in TPM?
Licensed fee-for-service physicians providing longitudinal community-based family medicine in Saskatchewan.
How do I enrol in TPM?
Eligible physicians must register to participate in TPM.
How do I make changes, updates or withdraw from TPM registration?
Changes to your registration can be made by sending an email to: tpm@health.gov.sk.ca.
Is TPM mandatory? If I join, can I leave it?
The TPM is voluntary. Family physicians are free to join or withdraw from the program. If you wish to withdraw from the program, please send an email detailing the following information to tpm@health.gov.sk.ca:
- Physician Number
- Physician Name
- Date of Withdrawal
Please note that payment will not occur if your request for withdrawal takes place within the first quarter of the program.
Can solo practice physicians enrol in TPM?
Solo practice does not exclude a physician from joining TPM. As part of the commitment to transition towards the Patient's Medical Home framework, physicians are expected to join a group (two or more) to share information from cross coverage, establish a call group and identify a group lead to support capacity building initiatives for clinics. Physicians can meet this commitment and remain an independent practice (see TPM Deliverables).
I understand that I must have SHA appointment/privileges to be eligible for TPM. How do I obtain an SHA appointment privileges?
Please contact the SHA to inquire about the process:
- Saskatoon – Ashley.mann@saskhealthauthority.ca
- Regina – shaphysiciancareersregina@saskhealthauthority.ca
- North East – Deborah.wick@saskhealthauthority.ca
- North West – angela.bodnar@saskhealthauthority.ca
- South East – psa-southeast@saskhealthauthority.ca
- South West – PSA-SouthWest@saskhealthauthority.ca
Patient Contact
What type of primary care services count towards patient contacts?
Services associated with the delivery of longitudinal community-based family medicine count as patient contacts including GP visit services, prenatal and infant services, some minor procedures (e.g., suturing, other minor treatments not billed with a visit code), and some in-office diagnostics (e.g., ECG, spirometry).
Please contact pmh@sma.sk.ca if you have questions regarding the inclusion of specific services.
If I see the same patient more than once in a day, does it count as more than one contact?
No, contacts counts are limited to one per day per patient.
Why are hospital care codes (25B - 28B) not included in patient contacts?
TPM provides additional compensation for community-based longitudinal care for services that include contact with a patient.
Hospital care remains an important service provided by family physicians, particularly in rural areas of the province. The new physician services agreement addresses the value of these services by including a new 15% premium to fee codes for services delivered in rural Saskatchewan, which are in addition to significant increases to hospital care fee codes (25B-28B) that occurred as part of the April 2024 allocation process.
Patient Panel
Where can I get my Health Quality Council (HQC) patient panel report?
Your panel report is available at Physicians Practice Report.
Why does my panel noted in the HQC patient panel report differ from the panel used to determine my TPM payment?
The panel methodology used the determine the TPM payment includes Nurse Practitioners and excludes clinics that do not primarily practice longitudinal family medicine. Information specific to payment drivers, deliverables and clinic activities will be available through your TPM report (currently in development).
How often is my patient panel calculated?
Patient panels are calculated semi-annually in April and October of each year.
Is there a limit on the number of empaneled patients a physician may have?
There is no limit on the number of empaneled patients a physician may have; however, to be eligible for TPM, a physician must have a minimum panel size of 250.
In determining panel size, are there special considerations for physicians who do not have three full years of consecutive billings?
The panel size methodology is adjusted to reflect the following special circumstances:
- Physicians new to practice and/or new to Saskatchewan.
- Physicians intending to shift their practice to focus primarily on longitudinal community-based family medicine.
- Physicians who have taken a leave of absence greater than 6 months within the panel size assessment period.
How will panel sizes be determined for family physicians new to practice and/or new to Saskatchewan?
As an incentive for new family physicians choosing to practice in Saskatchewan, the below panel sizes will be used to inform payment for family physicians in the first two years of practice.
| Range of Contacts | Year 1 | Year 2 |
| 0-749 | 0 | 0 |
| 750-1,999 | 640 | 715 |
| 2,000-2,999 | 745 | 830 |
| 3,000-3,999 | 850 | 950 |
| 4,000-4,999 | 980 | 1,095 |
| 5,000+ | 1,065 | 1,190 |
The panel size used is directly correlated with the physician’s activity level (as measured by patient contacts).
How will panel size be determined for Physicians intending to shift their practice to focus primarily on longitudinal community-based family medicine?
Panel size will be determined using the same methodology that was established to support physicians new to practice and/or new to Saskatchewan.
The physician’s activity level (as measured by patient contacts) will be used to determine the appropriate panel size based on the following table.
| Range of Contacts | Year 1 | Year 2 |
| 0-749 | 0 | 0 |
| 750-1999 | 640 | 715 |
| 2000-2999 | 745 | 830 |
| 3000-3999 | 850 | 950 |
| 4000-4999 | 980 | 1,095 |
| 5000+ | 1,065 | 1,190 |
If you are a family physician wishing to shift your area of practice to support longitudinal community-based family medicine, please contact us at tpm@health.gov.sk.ca
How is panel size determined for a family physician who has been on a leave of absence (greater than six consecutive months) within the 4-cut methodology assessment period?
The physician will receive the greater panel size as determine between the 4-cut methodology and the panel size associated with the physician’s activity level as noted in table below:
| Range of Contacts | Panel Size |
| 0-749 | 0 |
| 750-1999 | 750 |
| 2000-2999 | 875 |
| 3000-3999 | 1,000 |
| 4000-4999 | 1,150 |
| 5000+ | 1,250 |
This methodology will only apply in circumstances where a leave of absence is beyond the control of the physician (i.e., medical leave of absence, maternity/paternity leave).
If you experience a leave (greater than six months) at any point following your registration to TPM, please contact us at TPM@health.gov.sk.ca.
Payment
When will I receive my first payment?
It is anticipated that the first quarter payment will be made on August 26, 2024.
How often will payments occur?
TPM payment calculations occur quarterly; Following the first quarter payment, payments will be provided to participating physicians within 30 days of the end of the quarter.
Is there a maximum amount paid in each quarter?
The maximum annual payment a family physician can receive through TPM is $144,000 per fiscal year. To support the administrative process and provide timely payments to physicians, the maximum annual eligible amount will be divided into four quarters ($36K each quarter).
To account for fluctuations in the volume of services between quarters and to ensure all billing services are included, a reconciliation process will occur six months after the end of each fiscal year. An additional payment not to exceed $144,000 may result from the reconciliation process.
Will the TPM calculation include patient complexity modifiers?
Patient complexity modifiers are not used to calculate payments in the current methodology. However, the Ministry of Health and SMA intend to jointly review and develop patient complexity modifiers for future payment calculations.
How will the payment be made to me?
Deposits will be made automatically in accordance with your payment information as registered with the Medical Services Branch at the Ministry of Health.
Can I choose which account my payment is deposited to?
The payment will be made automatically in accordance with the following priority sequence:
- We pay to the professional corporation first.
- If there is no professional corporation, we pay to the solo clinic.
- If there is no solo clinic, we pay to the clinic with the highest payments in the last quarter.
Patient Matching
How are Saskatchewan residents matched to a family physician using a four-cut method?
Residents are matched to one provider using a four-cut method:
- Cut 1: Saw only you. If an individual only saw you during the three years, they are matched to you. Otherwise, go to cut 2.
- Cut 2: Saw you the majority of the time. If an individual saw you and other providers, but visited you the majority of the time, they are matched to you. Otherwise, go to cut 3.
- Cut 3: Had their last physical examination with you. If an individual saw you and other providers the same number of times, they are matched to you if you did the last physical exam (fee codes: 3B, 4B, 52B, 64B). Otherwise, go to cut 4.
- Cut 4: Saw you last. If an individual saw you and other providers the same number of times and has not had a physical, they are matched to you if they saw you last.
Note: Providers in the four-cut method include family physicians and nurse practitioners. Patients who match to an NP will not be matched to a FP.
What are the other inclusion and exclusion criteria for the patient matching?
Every Saskatchewan beneficiary with a billed service to an in-province Family Physician or Nurse Practitioner practicing at a Family Medicine or Primary Health Clinic is matched to one provider. Patients matched to providers are added to create the total panel size.
Inclusion Criteria
i) Patients are matched to a provider working at a clinic that was determined to offer full-service primary care services by an Family Physician or Nurse Practitioner.
ii) A full-service family medicine or primary care clinic is defined as a clinic that offers routine care, care for urgent but minor or common health problems, minor mental health care, maternity and childcare, liaison with home care, health promotion and disease prevention, nutrition counselling and end-of-life care.
iii) Patients are defined as Saskatchewan beneficiaries for which a billable service was submitted to MSB by a Family Physician or Nurse Practitioner at a primary care clinic during the three-year analysis period.
Other
Do I need to add all services for comprehensive care to qualify for TPM?
As part of TPM, physicians are expected to provide comprehensive care, including hospital and supportive care, nursing home care, pre- and post-natal and infant care, complete physicals (including PAP smears), and phone calls from Allied Health Care Providers (AHCP), where applicable.
The Ministry will continue to monitor the use of billing codes as part of the Family Physician Comprehensive Care Program (FPCCP). If a clinic is meeting most of the requirements of comprehensive care, and currently qualifies for compensation under FPCCP, a physician will not need to add additional services.
If I am a physician wishing to shift my area of practice to focus primarily on longitudinal community-based family medicine, how do I register for TPM?
Please email the TPM team at tpm@health.gov.sk.ca to express your interest and intention to make these changes.
The TPM team will then provide guidance on how to register for the TPM program.
Is care provided to out-of-province patients a factor in determining my contacts and/or my panel size?
Care provided to out-of-province patients is excluded from both patient contacts and panel size calculations.
Why is chronic disease management required as part of TPM?
In registering for TPM, physicians are required to commit to provide chronic disease management that aligns with best practices, ensuring patients living with chronic conditions receive the very best care.
To bill chronic disease fee codes (64B-68B), best practices in chronic disease management must be met, including the completion of CDM-QIP flowsheets. A description of these fee codes and the associated requirements can be found in the Physician Payment Schedule.
Information regarding the Chronic Disease Management Quality Improvement Program (CDM-QIP) including the required flow sheets can be found on the following eHealth website: CDM
I currently receive CDM-QIP and FPCCP payments. Will these payments continue?
Physicians enrolled in the TPM will no longer receive payments for FPCCP, Metro On-Call, and the CDM-QIP payment (specifically, the $75 payment for all indicators met per patient and per chronic condition in a 12-month period flow sheet). Fee for services payments for these services will continue.
Will payment for FPCCP and Metro On-Call be provided for the time prior to registering for TPM?
Yes, a pro-rated payment will be provided to account for any comprehensive care and on-call services delivered prior to joining TPM. Payments will reflect the time leading up to the start of the quarter in which a physician joins TPM.
If I register for TPM in the first quarter (April-June 2024), will I still receive FPCCP and Metro On-Call payment for the period of January-March 2024?
Yes, a prorated payment will be provided to account for any comprehensive care and on-call services prior to April 1, 2024. This also applies if a physician chooses to sign up in a later quarter; payment will reflect the time leading up to the start of the quarter in which the physician joins TPM.
How will FPCCP and Metro On-Call payments be calculated within a clinic if some physicians are registered for TPM and others are not?
The Ministry will continue to monitor clinic activity and the requirements under FPCCP. Physicians eligible for FPCCP will continue to receive payments based on clinic activities.
Why do I have to consent to share my data?
Participation in TPM requires that a physician commits to necessary data tracking, sharing and reporting that demonstrates improvements to longitudinal community-based family medicine delivery and patient outcomes as jointly developed by the Ministry of Health and the SMA.